FH is an inherited condition, but it is manageable when diagnosed early. If the patient has not shown any clinical symptoms, prevention of primary manifestation is prioritized. Otherwise, treating and mitigating further complications should be the focus.1
The treatment goals are2
to reduce the cumulative burden of elevated LDL-C levels
to control/ mitigate the development of further cardiovascular diseases
GUIDELINE
RECOMENDATIONS3
Assessment for cardiovascular
disease (CVD) risk
Systematic global CVD risk assessment is recommended to guide treatment decision-making. Individuals with FH are at high- or very-high risk of CVD. To improve risk assessment, the use of imaging techniques to detect asymptomatic atherosclerosis is recommended.
Very high risk
High risk
FH patients with
atherosclerotic cardiovascular disease (ASCVD) or
another major risk factor such as a calculated
SCORE
≥ 10% for 10-year risk of fatal CVD, DM with target organ damage, etc.
LDL-C < 55 mg/dL AND
≥ 50% LDL-C reduction from baseline*
LDL-C < 70 mg/dL AND
≥ 50% LDL-C reduction from baseline*
* Baseline refers to the LDL-C level in a person not taking any lipid-lowering therapy or to the extrapolated baseline value for those who are on current treatment.
TREATMENT OPTIONS
FH management is composed of non-pharmacological and pharmacological elements.
Non-pharmacological: dietary, lifestyle modifications and smoking cessation2
Systematic global CVD risk assessment is recommended to guide treatment decision-making. Individuals
with FH are at high- or very-high risk of CVD. To improve risk assessment, the use of imaging techniques
to detect asymptomatic atherosclerosis is recommended.
Lifestyle interventions to reduce LDL-C level 3
Magnitude of the effect
Avoid dietary trans fats
Reduce dietary saturated fats
Increase dietary fibre
Use functional foods enriched with phytosterols
Use red yeast rice nutraceuticals
Reduce excessive body weight
Reduce dietary cholesterol
Increase habitual physical activity
Some food choices to help lower LDL-C and improve the overall lipid profile
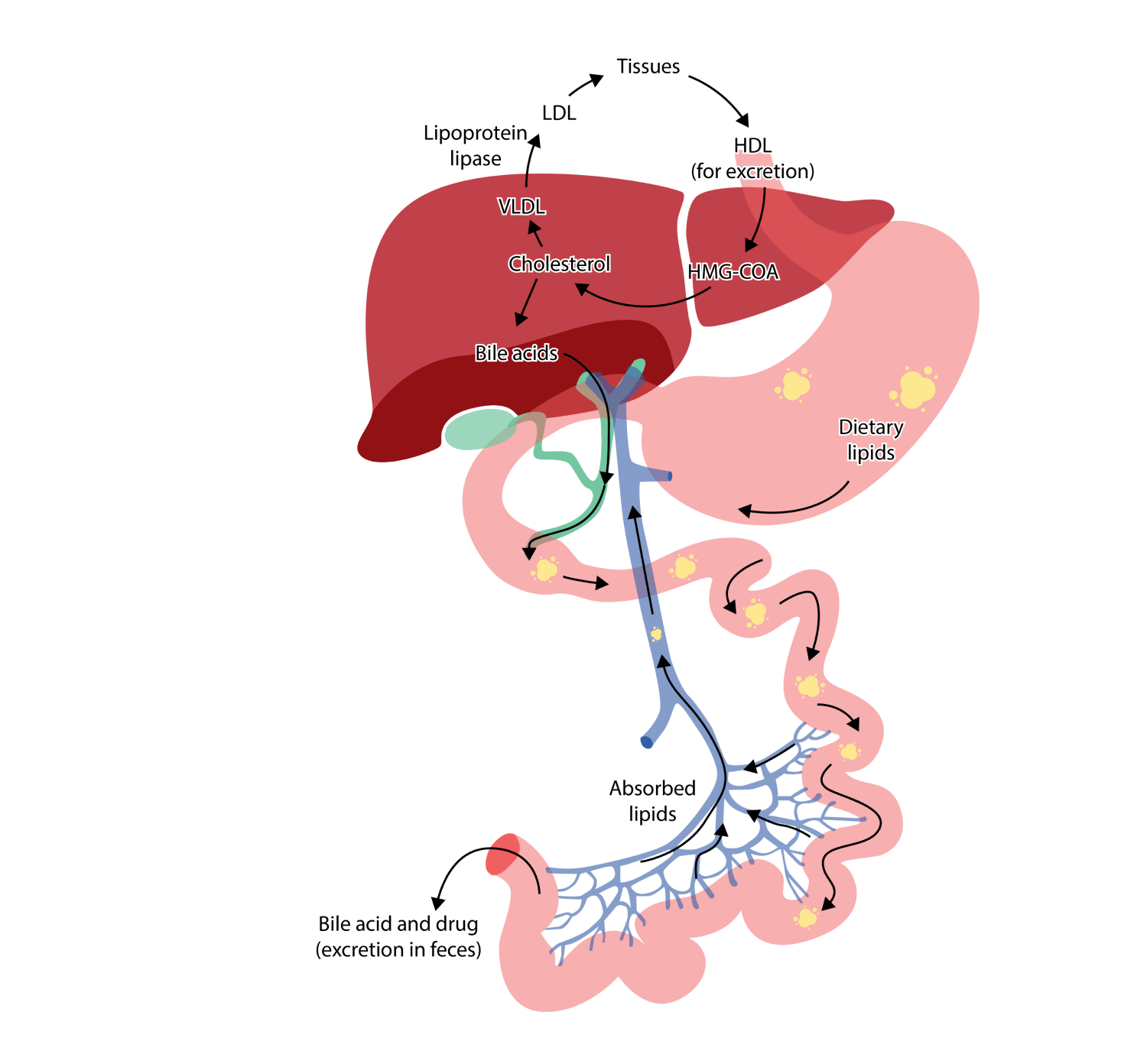
FH management is composed of pharmacological and non-pharmacological elements.
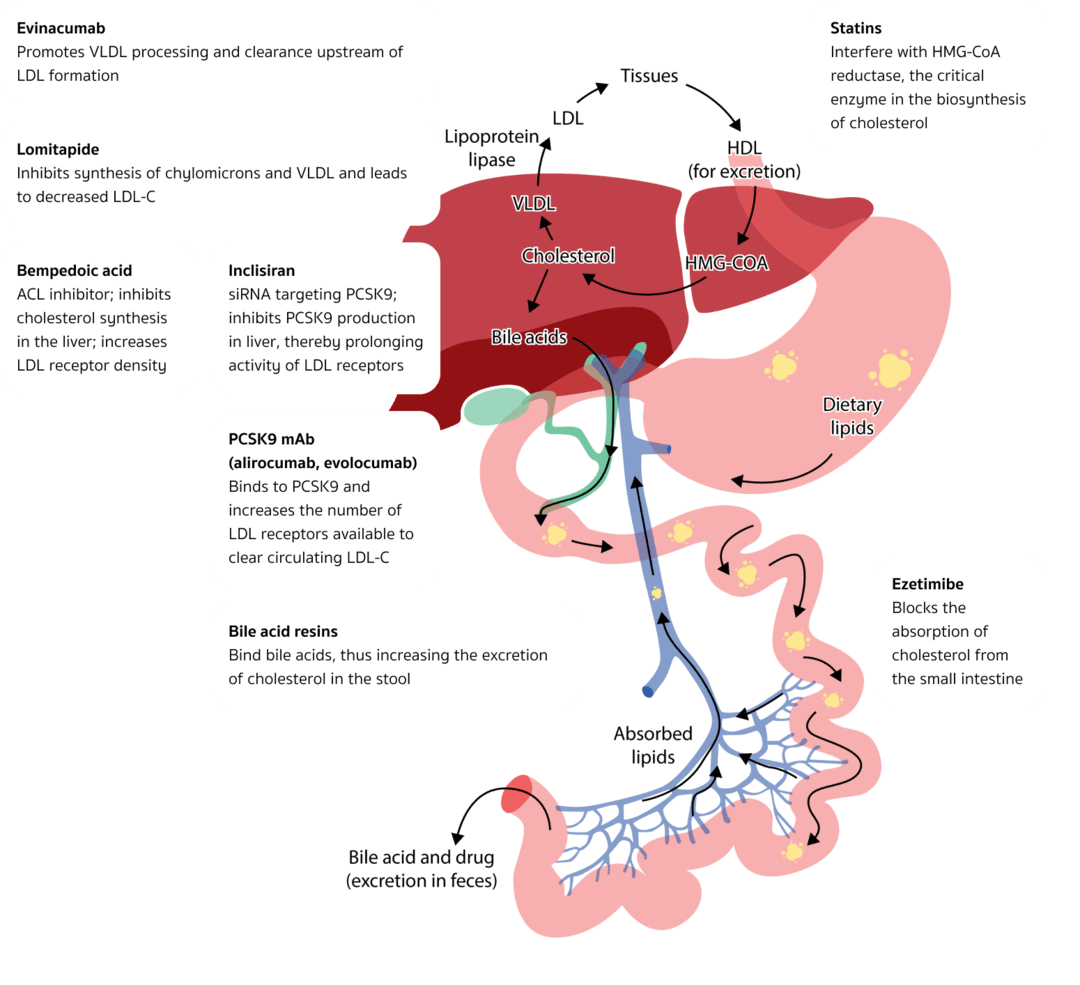
LDL-C lowering mechanisms.4,5
Evinacumab
Promotes VLDL processing and clearance upstream of LDL formation
Lomitapide
Inhibits synthesis of chylomicrons and VLDL and leads to decreased LDL-C
Statins
Interfere with HMG-CoA reductase, the critical enzyme in the
biosynthesis of cholesterol
Bempedoic acid
ACL inhibitor; inhibits cholesterol synthesis in the liver; increases
LDL receptor density
Inclisiran
siRNA targeting PCSK9; inhibits PCSK9 production in liver, thereby
prolonging activity of LDL receptors
PCSK9 mAb (alirocumab, evolocumab)
Binds to PCSK9 and increases the number of LDL receptors available to
clear circulating LDL-C
Bile acid resins
Bind bile acids, thus increasing the excretion of cholesterol in the
stool
Ezetimibe
Blocks the absorption of cholesterol from the small
intestine
Cholesterol-lowering treatment should be initiated as soon as possible after a diagnosis has been made.
Treatment should be initiated with high-intensity statin therapy, in most cases in combination with
ezetimibe.3,5
LDL-C < 55 mg/dL AND
≥ 50% LDL-C reduction from baseline*
High risk
LDL-C < 70 mg/dL AND
≥ 50% LDL-C reduction from baseline*
LDL-C <135 mg/dL
at >10 years of age
Statins
Recommended (often in combination with ezetimibe)
Recommended (often in combination with ezetimibe)
Recommended(start from age 8 to 10 as long as proved safe for children)
Should be started with low doses and the dose should be increased to reach goals
Non statin therapies: 1st consider ezetimibe and/or PCSK9 mAbs 2nd May consider bempedoic acid or inclisiran 3rd May consider evinacumab, lomitapide and/or lipoprotein apheresis
Ezetimibe
Recommended (often in combination with statin)
Recommended (often in combination with statin)
PCSK9 mAbs*
If
The treatment goal is not achieved on maximal tolerated statin plus ezetimibe for
very-high-risk patients
FH patients who cannot tolerate statin
Consider PCSK9 inhibitor with or without apheresis
PCSK9 inhibitor is not recommended in patients with LDLR-/- mutations (LDLR activity <
2%)
According to ACC 2023 expert consensus, Recommend PCSK9 (evolucumab) in
patients ≥ 10 years with HeFH as an adjunct to diet and other LDL-C
lowering therapies
Other
May consider bempedoic acid or inclisiran5
May consider evinacumab, lomitapide, and/or lipoprotein
apheresis for HoFH under care of lipid specialist5
HeFH: ezetimibe, bile acid-binding resin
HoFH: lipoprotein apheresis (by age 5 and not later than 8 years)
* PCSK9 mAbs5: alirocumab and evolocumab
REFERENCES:
Ison HE, et al. Familial Hypercholesterolemia. 2014 Jan 2 [Updated 2022 Jul 7]. In: GeneReviews®. Seattle (WA): University of Washington, Seattle. Available from: https://www.ncbi.nlm.nih.gov/books/NBK174884/
Lui DTW, et al. Management of Familial Hypercholesterolemia: Current Status and Future Perspectives. J Endocr Soc. 2020;5(1):bvaa122.
Mach F, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111-188.
Nurmohamed NS, et al. New and Emerging Therapies for Reduction of LDL-Cholesterol and Apolipoprotein B: JACC Focus Seminar 1/4. J Am Coll Cardiol. 2021;77(12):1564-1575.
Writing Committee; et al. 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2022;80(14):1366-1418.
Catapano AL, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016;253:281-344.
Landmesser U, et al. European Society of Cardiology/European Atherosclerosis Society Task Force consensus statement on proprotein convertase subtilisin/kexin type 9 inhibitors: practical guidance for use in patients at very high cardiovascular risk. Eur Heart J. 2017;38(29):2245-2255.
Cuchel M, et al. 2023 Update on European Atherosclerosis Society Consensus Statement on Homozygous Familial Hypercholesterolaemia: new treatments and clinical guidance. Eur Heart J. 2023;44(25):2277-9
Nordestgaard BG et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013; 34:3478a-3490a.

 ≥ 10% for 10-year risk of fatal CVD, DM with target organ damage, etc.
≥ 10% for 10-year risk of fatal CVD, DM with target organ damage, etc.
 Wholegrains
Wholegrains Vegetables
Vegetables Legumes
Legumes Fresh or frozen fruit
Fresh or frozen fruit Lean and oily fish,
Lean and oily fish, Skimmed milk and
Skimmed milk and Vinegar, mustard,
Vinegar, mustard,